Bisphosphonates “-dronates”
Considered as primary prevention of osteoporosis + first-line pharmacological treatment for post-menopausal women at risks of fractures
Route: IV/oral (frequency monthly~yearly depending on specific drug)
Mechanism of action:
- High affinity to and binds to hydroxyapatite in bone (mineralised form of calcium), Incorporation into bone matrix
- Taken up by osteoclasts during resorptions → inhibit osteoclast bone resorptions
- Effects persist post-treatment
Two classes of bisphophonates:

Indications:
- Osteoporosis
- Paget’s Disease – abnormal bone remodelling leading to overly
- fragile bones
- Metastatic bone disease –
- Hypercalcemia
- Prevention of fractures

Mechanism of action of bisphosphonates;
Reference: Schmidt GA, Horner KE, McDanel DL, Ross MB, Moores KG. Risks and benefits of long-term bisphosphonate therapy. American Journal of Health-System Pharmacy. 2010 Jun 15;67(12):994–1001.
Adverse drug effects:
- Oral route – Upper GI side effects
- Oesophagitis
- Oesophageal erosion
- Gastritis
- Minimised by taking drug with water and staying upright
- IV route
- Osteonecrosis of jaw
- Myalgia
- Hypocalcaemia
- Limited evidence of osteoprotective after 5 years
RANK Ligand Inhibitors – Denosumab
Humanised monoclonal Ab
Route: IV or SC at least 6 monthly
Mechanism of action:
- Binds to RANKL to inhibit activation of RANK receptors on osteoclasts
- Prevents/reduces RANK/RANKL mediated osteoclast differentiation, survival and activity
- Limits bone resorption
- Decreases bone turnover markers and increases bone density
- Effects do not persist post-treatment
Indications:
- Post-menopausal OP (IV every 6/12)
- Bone metastases (IV every 1/12)
- Fracture prevention in GC usage
ADEs:
- Hypocalcaemia + hypophosphotemia
- Osteonecrosis of jaw
- Myalgia
- Infection (inhibition of RANKL immune modulation)
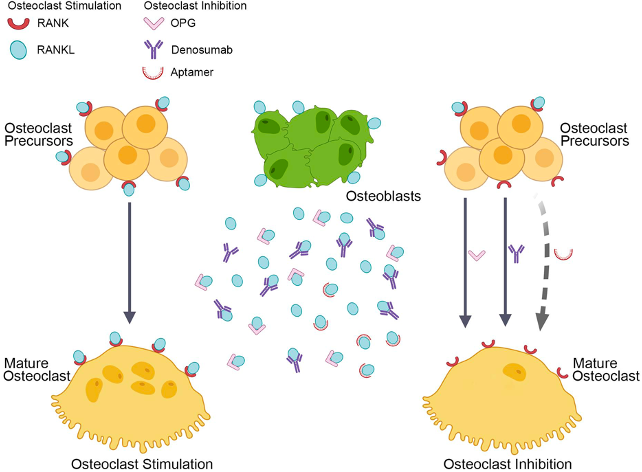
Mechanism of action of RANKL inhibitors;
Reference: Zhang N, Zhang ZK, Yu Y, Zhuo Z, Zhang G, Zhang BT. Pros and Cons of Denosumab Treatment for Osteoporosis and Implication for RANKL Aptamer Therapy. Frontiers in Cell and Developmental Biology. 2020 May 14;8.
Calcitonin Analogues – Salcatonin (salmon calcitonin)
Route: SC, IM or nasal spray
MoA:
- Binding to osteoclast calcitonin receptors
- Direct inhibition of osteoclast activity → ↓ bone resorption
- Stimulates bone growth by activity on osteoblasts
- ↑ Excretion of Ca2+ and PO43- by activity on kidneys
Indications:
- Post-menopausal or GC induced OP
- Hypercalcaemia
- Paget’s disease of bone

Mechanism of action of calcitonin;
Reference: Aleksic A. Calcitonin (Miacalcin) Uses & Side Effects [Internet]. SelfHacked. 2019. Available from: https://selfhacked.com/blog/calcitonin-miacalcin/
Selective Oestrogen Receptor Modulator (SERM) – Raloxifine
Route: daily oral
MoA:
- Partial agonist in oestrogen receptor of bones
- Osteo-protective by stimulating osteoblast activity
- Antagonist at oestrogen receptor in mammary and uterine tissues
Indications:
- OP prevention in post-menopausal women (especially with
- breast ca. + FHx of breast ca.)
- Breast cancer prevention
ADEs:
- Hot flushes (lesser of extent than oestrogen selectivity)
- ↑ Risk of venous thrombosis events (DVT, PE)

Mechanism of action of SERMs, where bone action is via agonist pathway;
Reference: Duarte FH, Jallad RS, Bronstein MD. Estrogens and selective estrogen receptor modulators in acromegaly. Endocrine. 2016 Oct 4;54(2):306–14.
Calcimimetic Agents – Cinacalcet
Allosteric modulator of calcium sensing receptor (CaSR) on parathyroid glands
Route: Oral QID (low bioavailability)
MoA:
- Increases activation of CaSR
- Suppression of PTH release → suppresses osteoclast activity
- Reduction of serum [Ca2+]
Indication:
- Hypercalcaemia in parathyroid carcinoma
- 1° Hyperparathyroidism
ADEs:
- Hypocalcaemia, paraesthesia, myalgia
- Increased clearance with tobacco use (via CYP450)

Mechanism of action of calcimimetics;
Reference: Mazzaferro S, Pasquali M. Direct bone effects of calcimimetics in chronic kidney disease? Kidney International. 2019 May;95(5):1012–4.
References:
- Aleksic, A. (2019, October 28). Calcitonin (Miacalcin) Uses & Side Effects. SelfHacked. https://selfhacked.com/blog/calcitonin-miacalcin/
- Duarte, F. H., Jallad, R. S.,& Bronstein, M. D. (2016). Estrogens and selective estrogen receptor modulators in acromegaly. Endocrine, 54(2), 306–314. https://doi.org/10.1007/s12020-016-1118-z
- Mazzaferro, S., & Pasquali, M. (2019). Direct bone effects of calcimimetics in chronic kidney disease? Kidney International, 95(5), 1012–1014. https://doi.org/10.1016/j.kint.2019.01.045
- McCarty, R. (2023). Drugs used to treat bone disorders. University of Melbourne MD1 MSK Lecture.
- Schmidt, G. A., Horner, K. E., McDanel, D. L., Ross, M. B., & Moores, K. G. (2010). Risks and benefits of long-term bisphosphonate therapy. American Journal of Health-System Pharmacy, 67(12), 994–1001. https://doi.org/10.2146/ajhp090506
- Vasiljević, F., & Florjanczyk, U. (2018, October 7). Osmosis: Osteoporosis medications (S. Gillespie & Y. Xiao, Eds.). Osmosis. https://www.osmosis.org/learn/Osteoporosis_medications
- Zhang, N., Zhang, Z.-K., Yu, Y., Zhuo, Z., Zhang, G., & Zhang, B.-T. (2020). Pros and Cons of Denosumab Treatment for Osteoporosis and Implication for RANKL Aptamer Therapy. Frontiers in Cell and Developmental Biology, 8. https://doi.org/10.3389/fcell.2020.00325
Authors
Kevin Li, medical student MD2, Western Health 2024
Matthew Sun, orthopaedic resident, Western Health 2024